Our milestone accomplishments for the past year include:
- Exploring new approaches for helping to stabilize lax and unstable joints
- Developing novel treatment strategies for symptoms associated with dysautonomia
- Strategies to relieve symptoms and treatment for postural orthostatic tachycardia syndrome
- Exploring methods for minimizing symptoms of gastroparesis
- Evaluating surgical strategies to stabilize problematic joints associated with debilitating pain
Our Current Study
Using cheek swabs or blood from families with a history of hypermobile EDS (also known as hEDS or EDS Type III), we are collecting DNA for next-generation sequencing. We completed analyzing the data of next-generation sequencing in 26 subjects and we are trying to confirm the results by using Sanger sequencing. Our promising preliminary results showed several gene variations were associated with bone fracture, tendon-ligament injury, muscle pain (myalgia) and skin fragility in the EDS patients.


Our goal: To identify the gene mutations associated with EDS type III that cause this common genetic disorder. We plan to create a diagnostic genetic panel for hEDS.
Our challenge: Genetic evaluation is costly. With so many patients now realizing they have EDS, we are currently collecting more than 300 DNA samples from affected and unaffected family members. In order to conduct the expensive genetic analysis in all of the samples we can only do it with your help.
Published Research
-

Review
By Purusha Shirvani, Arash Shirvani and Michael F. Holick
February 19, 2025
-

Case Report
By Arash Shirvani, Purusha Shirvani, Ugochukwu Jonah, Brian E. Moore and Michael F. Holick
February 14, 2025
-

Article
By Nazlı Uçar and Michael F. Holick
January 22, 2025
Abstract
Sunlight exposure plays an important role in human health, impacting processes such as mood, blood pressure regulation, and vitamin D3 production. Solar ultraviolet B radiation initiates vitamin D3 synthesis in the skin, which is subsequently metabolized into its biologically active form. UVB exposure plays a key role in enabling vitamin D3 synthesis, but it can also contribute to skin carcinogenesis, creating a complex interplay between its beneficial and harmful effects.
Vitamin D deficiency, affecting over half the global population, is linked to a range of chronic diseases, including cancers, cardiovascular conditions, and autoimmune disorders. Simultaneously, excessive solar UVB exposure increases the risk of non-melanoma and melanoma skin cancers through mechanisms involving DNA damage and oxidative stress.
This review examines the dual role of UVB radiation in health and disease, focusing on the mechanisms of cutaneous vitamin D3 synthesis, the epidemiology of skin cancer, and the protective roles of vitamin D3’s photoproducts and its active metabolite, 1,25-dihydroxyvitamin D3. Understanding these interconnections is critical for developing strategies that balance adequate sun-induced vitamin D3 production with skin cancer prevention.
-


Article
By Michael F. Holick PhD, MD
October 30, 2024
Background/Objective
The goal of this review is to compare the 2024 and 2011 Endocrine Society’s Clinical Practice Guidelines on vitamin D2 or vitamin D3 (vitamin D). The 2024 Guideline made recommendations for the general healthy population for skeletal and extra skeletal health benefits of vitamin D. This contrasts with the 2011 Guidelines which provided clinicians with guidance on how to evaluate and treat patients with vitamin D deficiency and prevent recurrence.
Discussion
The 2024 Guideline focused on randomized controlled trials and ignored association studies and other studies that have supported the skeletal and extra skeletal health benefits of vitamin D. The 2024 Guideline recommended empiric vitamin D in children and adolescents aged 1 to 18 years to reduce risk of upper respiratory tract infections, pregnant women to improve pregnancy-related outcomes, prediabetic patients to reduce risk of diabetes, and to improve mortality in those over 75 years.
Conclusion
These guidelines do not apply to individuals with abnormalities in calcium, phosphate, vitamin D, and bone metabolism which were provided in the 2011 Guidelines. For nonpregnant adults up to the age of 75, they recommend the Dietary Reference Intakes of 600 IUs (international units; 1 IU = 25 ng of vitamin D), and 800 IUs as recommended by The Institute of Medicine. Association studies have suggested that to obtain maximum extraskeletal benefits from vitamin D including reducing risk of upper respiratory tract infection for children and adults, autoimmune disorders, pre-eclampsia, low birth weight, neonatal dental caries, and deadly cancers circulating concentrations of 25-hydroxyvitamin D should be at least 30 ng/mL with a preferred range of 40-60 ng/mL as recommended by the 2011 Guidelines.
-
Article
By Purusha Shirvani, Arash Shirvani and Michael F. Holick
October 17, 2024
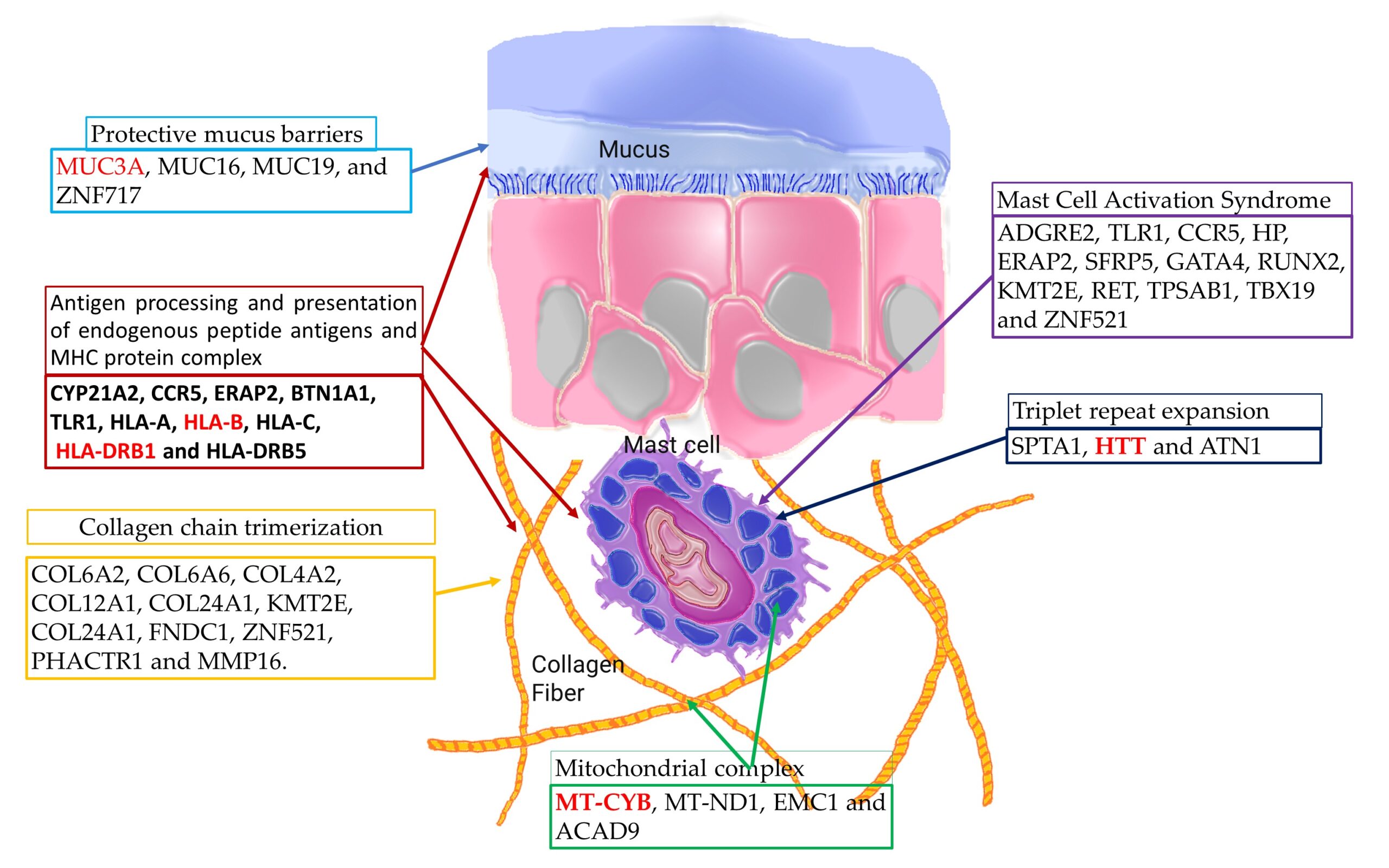
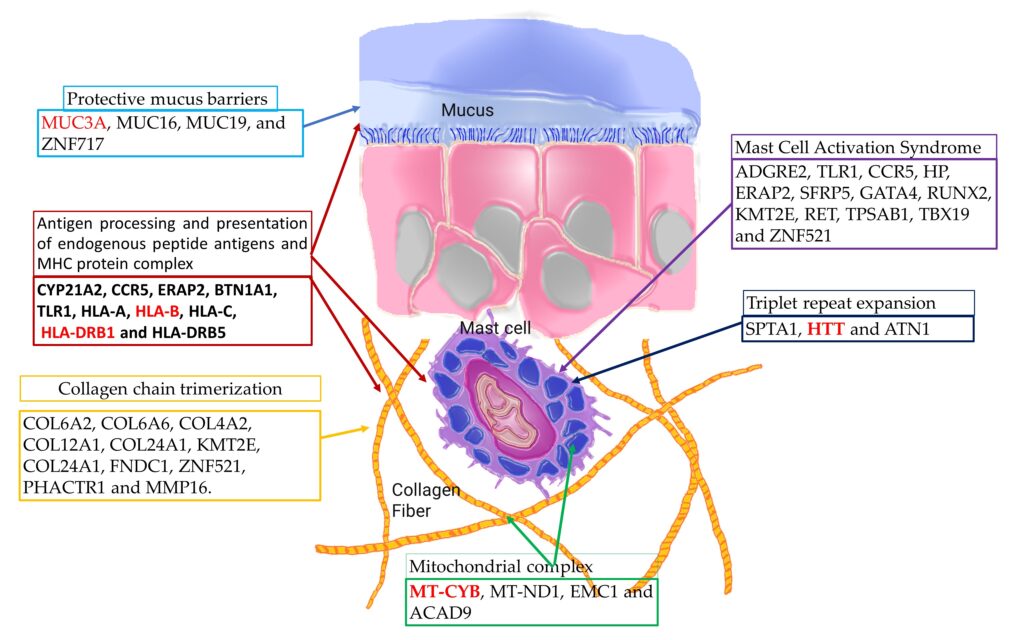
Hypermobile Ehlers-Danlos syndrome (hEDS) is a connective tissue disorder marked by joint hypermobility, skin hyperextensibility, and tissue fragility. Recent studies have linked hEDS with mast cell activation syndrome (MCAS), suggesting a genetic interplay affecting immune regulation and infection susceptibility. This study aims to decode the genetic basis of mast cell hypersensitivity and increased infection risk in hEDS by identifying specific genetic variants associated with these conditions.
We conducted whole-genome sequencing (WGS) on 18 hEDS participants and 7 first-degree relatives as controls, focusing on identifying genetic variants associated with mast cell dysregulation. Participants underwent clinical assessments to document hEDS symptoms and mast cell hypersensitivity, with particular attention to past infections and antihistamine response.
Our analysis identified specific genetic variants in MT-CYB, HTT, MUC3A, HLA-B and HLA-DRB1, which are implicated in hEDS and MCAS. Protein–protein interaction (PPI) network analysis revealed significant interactions among identified variants, highlighting their involvement in pathways related to antigen processing, mucosal protection, and collagen synthesis. Notably, 61.1% of the hEDS cohort reported recurrent infections compared to 28.5% in controls, and 72.2% had documented mast cell hypersensitivity versus 14.2% in controls.
These findings provide a plausible explanation for the complex interplay between connective tissue abnormalities and immune dysregulation in hEDS. The identified genetic variants offer insights into potential therapeutic targets for modulating mast cell activity and improving patient outcomes. Future research should validate these findings in larger cohorts and explore the functional implications of these variants to develop effective treatment strategies for hEDS and related mast cell disorders.
-

Case Report
By Michael F. Holick, Arash Shirvani and Nipith Charoenngam
April 15, 2021
(Boston)—An intrauterine fracture is a rare finding during routine prenatal imaging. This condition can be due to maternal trauma, genetic disorders of the skeleton, as well as other predisposing maternal metabolic and vascular disorders. Genetic disorders that have previously been reported to cause intrauterine fracture include brittle bone disease (osteogenesis imperfecta or OI), osteopetrosis, hypophosphatasia and Ehlers-Danlos syndrome (EDS).
Now for the first time, researchers from Boston University School of Medicine (BUSM) report a new genetic cause, unrelated to OI, for the 23 fractures that occurred in-utero to a mother with EDS hypermobility type.
EDS is a disease that weakens the bones and connective tissues of your body. It can make joints loose and skin thin and easily bruised. It also can weaken blood vessels and organs. There are 13 types of EDS. The most common, and generally considered the least severe, is hypermobile EDS (hEDS). While there are genetic tests for some subtypes of EDS, no genetic test has been developed for diagnosing hEDS.
Following the birth, the mom, infant and dad were enrolled in BUSM’s Ehlers-Danlos Clinical Research Program. After evaluation of the family, including documenting medical history and physical findings, DNA samples were taken from each of them. The DNA was evaluated and confirmed that the infant had no pathologic genetic mutations associated with OI. However, several new gene mutations including one gene, CCDC134, that has been identified as causing bone fragility, was identified in the infant.
According to the researchers, this case report clearly demonstrates that there is at least one other genetic cause for infantile fractures other than OI and child abuse (non-accidental trauma) that is associated with EDS. “Therefore we are recommending that the additional gene we identified as being the likely cause for this infant’s fractures, be included in the genetic panel for bone fragility and that careful consideration be given for other causes of infantile fractures other than OI and non-accidental trauma,” said corresponding author, Michael F. Holick, PhD, MD, professor of medicine, physiology and biophysics and molecular medicine at BUSM.
While acknowledging that child abuse is a serious problem that needs to be dealt with appropriately, Holick believes misdiagnosing child abuse can also have devastating long-term consequences for both the child and the parents. “If this infant were brought into the hospital with an upper respiratory tract infection at eight weeks of age, an x-ray of his chest would have revealed healing fractures of his arms and multiple healing fractures of his ribs. A skeletal survey would have revealed the healing fractures in both his legs. He would have been tested and found not to have OI, and therefore the diagnosis for the fractures would have been that they were caused by non-accidental trauma. The child would have been immediately removed from the care of his parents and the parents would have been accused of felony child abuse. It is hoped that this case report will now give reconsideration for diagnosing child abuse solely based on x-ray findings of a fracture or fractures with a negative genetic test for OI,” he said.
Holick stresses that by better understanding how this pathologic genetic mutation affects the skeleton to cause fractures provides the scientific community with the ability to develop new strategies for treatment. “We will be able to develop new approaches not only for treating bone fragility in infants with this genetic disorder, but also for treating bone brittleness associated with osteoporosis, which is associated with enormous cost both in terms of quality of life and medical expenses,” Holick said.
-


Research Paper
By M. F. Holick, A. Hossein-Nezhad & F. Tabatabaei
February 16, 2017
Child Abuse and Neglect (CAN) is a serious public health crisis that has major implications for the welfare of the child involved. Inflicted non-accidental skeletal injuries are the second most common manifestation of child abuse after soft tissue injuries. There are several genetic disorders and congenital defect conditions that have been associated with bone fragility and fractures that can be misdiagnosed as child abuse. Osteogenesis Imperfecta (OI) is the most common genetic abnormality associated with multiple unexplained fractures in an infant or child that can be misdiagnosed as child abuse. Moreover, rickets and Ehlers-Danlos/hypermobility syndrome (EDS), which are associated with normal or low bone density and increased bone fragility, can also result in X-ray findings that can be mistaken for child abuse.
EDS is a genetic disease that affects collagen synthesis and structure resulting in multisystem connective tissue involvement with twelve different subtypes. The clinical manifestations of EDS include skin hyperextensibility, skin fragility, joint hypermobility, muscle hypotonia, easy bruising, and mast cell hypersensitivity. Moreover, fragility fractures with normal or low bone density has been reported among both pediatric and adult patients with EDS. EDS has been reported in the literature to be misdiagnosed as CAN due to unexplained facial scars and skin lesions. It has also been reported that EDS can present with a congenital skull fracture at birth. To our knowledge there has been no reported cases in the literature that link non-accidental fractures among infants with EDS and OI/EDS. However, concerns regarding the likelihood of increased risk for fractures among infants with EDS and the OI overlap syndrome and the possibility for misdiagnosing CAN have been raised.
Rickets is a metabolic bone disease most commonly caused by vitamin D deficiency. This deficiency results in demineralization of the skeleton due to secondary hyperparathyroidism as well as a mineralization defect of newly laid down osteoid. Vitamin D also plays a critical role in chondrocyte maturation and as a result vitamin D deficiency results in growth plates that have abnormal mineralization and ossification. The poorly mineralized skeleton of a rachitic child increases risk for fragility fractures and has been reported to be misdiagnosed as CAN. Similar bone lesions can be seen on an X-ray in both vitamin D deficiency rickets and infants and children suspected of being abused making it difficult to differentiate between these two conditions. Moreover, these two conditions can be found simultaneously in one patient.
Classic Metaphyseal Lesions (CMLs), also referred to as corner fractures or bucket handle fractures, were first attributed to Caffey who noted unusual radiologic lucencies in the growth plates in the long bones in 6 infants born between 1925 and 1942 who presented with subdural hematomas. Originally it was concluded that this radiologic finding was caused by a small piece of bone that was avulsed and considered due to shearing forces on the fragile growth plate. As a result of this interpretation of this radiologic finding most pediatric radiologists and child abuse experts consider it to be pathognomonic for non-accidental trauma. However Kleinman et al who introduced the term metaphyseal lesion (now known as classic metaphyseal lesion;CML proposed that this radiologic lucency was not an avulsion but rather was due to a transplanar micro-fracture of unknown etiology. They also concluded that most bucket-handle lesions are not associated with displaced fractures but were in fact a result of a nonorthograde radiologic protection. These radiographic findings are often subtle and easily misinterpreted as fractures. These lesions can be found in infants and children with vitamin D deficiency rickets as well as in children with the collagen matrix genetic disorder OI.
Acquired and genetic disorders of bone, such as vitamin D deficiency and EDS, are quite common and may be overlooked in infants who present with rib or extremity fractures in various stages of healing at several skeletal sites including CMLs. The importance of recognizing these conditions is stressed as it may save these families from the horrific consequences of being considered a child abuser including loss of their child and their other children to adoption, the possibility of being incarcerated as a felon and having their names placed on the child abuse registry limiting their present and future employment possibilities.
We present 72 cases of infants who presented with multiple fractures. Most were evaluated along with their parents for evidence of acquired or inherited bone diseases.